Patient PrePay
First Name
*
Last Name
*
MRN
Last 4 Digits of SSN
*
Patient Date of Birth
*
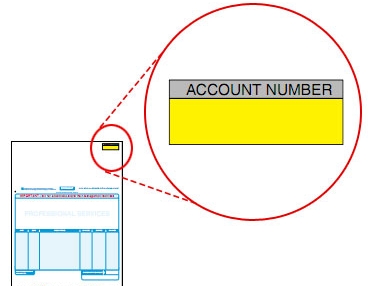
Account Number
Card Type
*
-- Select --
Credit
Debit
HSA
FSA
Card Network
*
--Select--
Master Card
Visa
Discover
Amex
Card Number
*
Name on Card
*
Expiration Date
*
MM
01
02
03
04
05
06
07
08
09
10
11
12
YYYY
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
2036
2037
2038
2039
2040
Date Of Service
CVV Number
*
Payment amount
*
Surcharge Amount
Total Amount
A non-refundable surcharge of % will be applied to this payment
Job Code
*
×
×